Architecture of an Arch: Why HOKAs can Comfort but Not Cure Plantar Fasciitis
- Candace

- Feb 8
- 7 min read
When looking at the bone structure of the human foot it is tempting to understand its structural integrity as comparable to that of a stone arch. It appears that the relationship between the bones is maintained by a balancing arrangement localized within the foot. But this is far from the truth.


The mechanics of the arch of the foot are far more like those of a suspension bridge. The integrity of the foot’s arch is determined by levels of tension maintained in “wires” that are anchored far above the foot itself.


To understand the function and dysfunction of the feet we must consider a picture that includes the rest of the body and its relationship to gravity. Further, in a case where an architectural arch or bridge is failing to function the solution would never be to fill up the space underneath the arch or cut a suspension wire, yet in the case of the arch of the foot these are thought to be appropriate resolutions to problems. Such an approach to the foot arch not only does not address the cause of the problem it facilitates the furtherance of the behaviors and misalignments that are the cause thereby worsening the problem.
Plantar Fasciitis is a term that describes inflammation (“itis”) of the fascia (connective tissue) of the plantar (bottom) surface of the foot. This term simply describes a condition associated with symptoms of inflammation which include pain, redness, swelling, and heat. Commonly anyone who has pain when they step down on their feet, whether on the heel or forefoot, and no other condition like degradation of cartilage, fracture or spurs has been identified is said to have this condition. The term Plantar Fasciitis says nothing about the cause of the inflammation, simply that inflammation exists.
The plantar fascia is largely identified with a structure called the plantar aponeurosis. You can see from the bottom and side angle that this connective tissue structure provides a band that prevents the collapse of the arch of the foot and when properly utilized stores energy for movement efficiency.


The plantar fascia does not exist as an isolated structure separate from the rest of the body. Every structure in the body from muscles and bones to organs and vessels are all wrapped with fascia and bound within a continuous, body-wide fascial or connective tissue system which includes tendons, ligaments, and aponeuroses. By way of this fascial system every structure within the body is connected to every other structure. Additionally, as our bodies and postural relationships with gravity develop, pathways are constructed across the length of the body by which tension can pull and force can move.
Imagine the incredibly complex mechanisms by which we manage to stand up right and move against the force of gravity. Our bodies are essentially a water bag held intact by pressure created through elastic banding and extended in length in opposition to gravity by suspending mineralized structures (bones) within this pressurized water bag. The suspension (not stacking) of bones is maintained by tension within muscles and connective tissue.
Now imagine how anything that stands upright from the earth must be stabilized with some sort of scaffolding along its entire length or it falls over. Our bodies achieve this through continuous tracts of connective tissue that span the length of the body along all sides and in spirals to facilitate stability through many directions of movement.

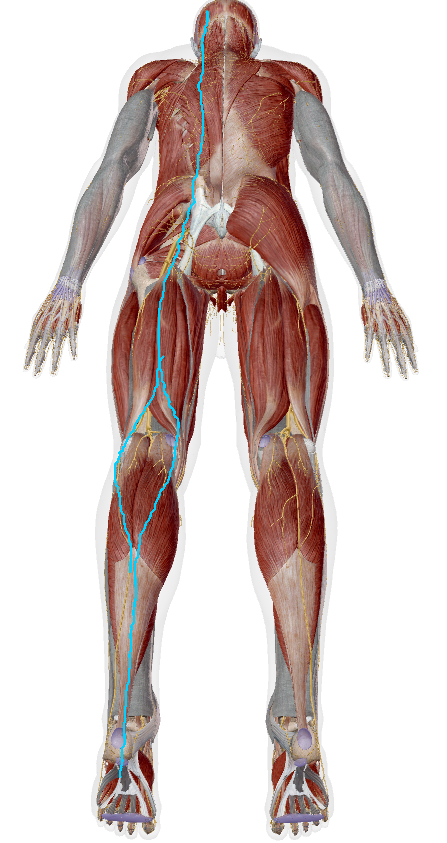
Thomas Myers has
done extensive work through many cadaver dissections teasing out the physical evidence of these pathways and has mapped them in a system that he calls Anatomy Trains. Based on his work, we can place the plantar fascia within a greater context as an end point of what Myers calls the Superficial Back Line. This line runs from the bottom of the toes, under the heel and up the Achilles tendon, through the calf and hamstrings, up the sacrotuberous ligament along the back of the pelvis, through the erector spinae muscles that run the length of the back and neck, and up over the head to end at the brow ridge just above the eyes. This means the level of tension, or amount of stretch available, in the plantar fascia is directly related to how tension is being distributed throughout the rest of the Superficial Back Line (SBL) spanning the entire length of the body. (1)
Now consider what happens when the SBL is too tight to allow the heel to properly touch the ground. Because the connective tissue band is continuous from far above the foot, to down over the end of the heel, and along the entire underside of the foot, movement of the heel toward the ground stretches this band in the same way the knee stretches the bands crossing over and around the patella to connect the tibia and femur when it bends. When the bands bridging the knee are too tight it restricts how far the knee can bend, the same is true of the heel. But in the case of the heel, we are at the end of the line available to draw stretch. So, when we force it to bend through contact with the ground farther than the tissue tension will allow the tissue can tear. Micro-tears in the plantar fascia trigger an inflammation response to stimulate repair, and voilà, plantar fasciitis.
There are three common scenarios that significantly distort the balance of tension

along the SBL and thereby negatively impact the plantar fascia. The first two are an increase in the curve of the upper back and an anterior tilt of the pelvis that both pull up the SBL. This upward pull tightens the slack or elasticity available down the rest of the SBL into the feet. These two postural distortions don’t always present together but often do as can be seen in the picture. Both are common consequences of prolonged sitting.
A third compounding factor is wearing shoes with a platform that elevates the heel above the forefoot which lifts the SBL and creates distortions in the ankle and foot. Consider the significance of the angle created by the ankle joint. In someone standing with proper alignment the ankle creates a close to 90-degree angle between the tibia and a flat, horizontal surface upon which the foot stands. This angle requires balanced muscle contractions between all sides of the leg to steady the position of the tibia in relation to the foot and a proper balance of flexibility and tension within the line of plantar fascia blending into the Achilles tendon to provide for proper stability while allowing enough stretch for the heel to rest on the ground.

Look at how elevating the heel above the forefoot to different heights affects the angle of the ankle, relationship of the position of the tibia to the ground, and the positional relationships between the bones of the feet.


Now consider the consequences of holding misaligned postures and distorted foot and ankle relationships over long periods of time. To understand the consequences of this one must understand the qualities of connective tissue itself. All connective tissue is composed of collagen fibers and a gooey ground substance. The relative amount of each and the arrangement of the collagen fibers determines what functional role that tissue will play. Bags that hold organs have a lot of ground substance and a low amount of collagen fibers that are loosely arranged. In comparison, ligaments and tendons have very little ground substance and a lot of densely packed collagen fibers. All connective tissue is both plastic and elastic. It provides for our tissue’s ability to rebound but also makes it possible for tissues to be remolded into a stable new arrangement. It does this by being able to shift from a softened to a hardened state and back again through the presence or absence of friction, pressure, or movement.
So, over time, tissues that are held continuously in a shortened position will become stuck at that length and no longer return to their originally designed length without intervention. Here is where the whole picture of plantar fasciitis really starts to form (in my non-medical opinion). It comes about as a combination of postural distortions, often compounded by footwear choices and fitness strategies that neglect to create alignment before adding weight and impact, that imbalance the tension along the SBL and leads to micro-tearing in the plantar fascia which triggers an inflammation response.
I hope that if you’ve made it this far it is already clear why putting a highly padded shoe, like a HOKA, under a foot that is inflamed will provide it comfort by maintaining an ankle angle that reduces stretch of the plantar fascia and buffers it from impact but that this won’t actually solve the cause of how it became inflamed in the first place. The causes lie somewhere above the feet in imbalances where muscles are not firing in equal opposition to each other on opposing sides of joints. Muscles and connective tissues are often stuck and shortened on one side of a joint and weak and over-stretched on the other. These imbalances affect how body weight is distributed over the feet and therefore its ability to absorb the force of impact with the ground.
Am I saying that to solve the problem of plantar fasciitis everyone should go out and buy barefoot shoes. Absolutely not! Am I saying to start building your core with a bunch of crunches and time on weight machines. Again, no.
What I’m hoping to make clear is that the proper functioning of the feet depends upon the proper alignment of the body over them. The foot and ankle are designed to act like a spring that can absorb the energy of impact and use it to help propel the body forward, but this design can’t function properly without the alignment of all the body’s major joints. Bringing joints back into alignment is not achieved through single plane movements with weights or static stretching. It comes through the slow, patient building of well-aligned micro-movements that increase mobility and flexibility through progressive multi-plane strength and balance challenges. You won’t look cool at the gym, but you’ll build a true foundation upon which to increase challenges and impact while maintaining long-term joint health.
So much more can be said, but this is a good place to stop for now. Let me know if what I’m saying is helpful.
(1) Anatomy Trains, Myofascial Meridians for Manual Therapists and Movement Professionals, Thomas W. Myers, 4th Edition, 2021 Elsevier Limited



Comments